![]()
In 2008, I published The Smart Mother’s Guide to a Better Pregnancy. Chapter 6 was about high blood pressure in pregnancy. I wrote it because I had watched too many women leave prenatal appointments without understanding what was happening inside their own bodies. I had reviewed too many cases where the warning signs were documented in the chart and still went missed.
I did not have a name for what I was seeing back then. I just knew that something was breaking down between what the evidence showed and what patients were told. Between what clinicians documented and what they acted on.
What I was describing, without yet knowing it, was a blindspot.
May is Preeclampsia Awareness Month. And this year, I want to mark it differently. Not with statistics alone. With a reckoning.
Here is what has changed since I wrote that chapter. And here is what has not.
What the Evidence Now Tells Us
The science has moved. Significantly. These are not minor updates. These are practice-changing shifts that every pregnant woman and every clinician needs to know.
Chronic hypertension is now treated earlier. If your blood pressure is 140 over 90, medication is recommended. Not 150 over 100. Not “let’s watch it.” The CHAP Trial in 2022 and updated ACOG guidance confirmed this. Earlier treatment reduces the risk of severe complications. This is a meaningful change.
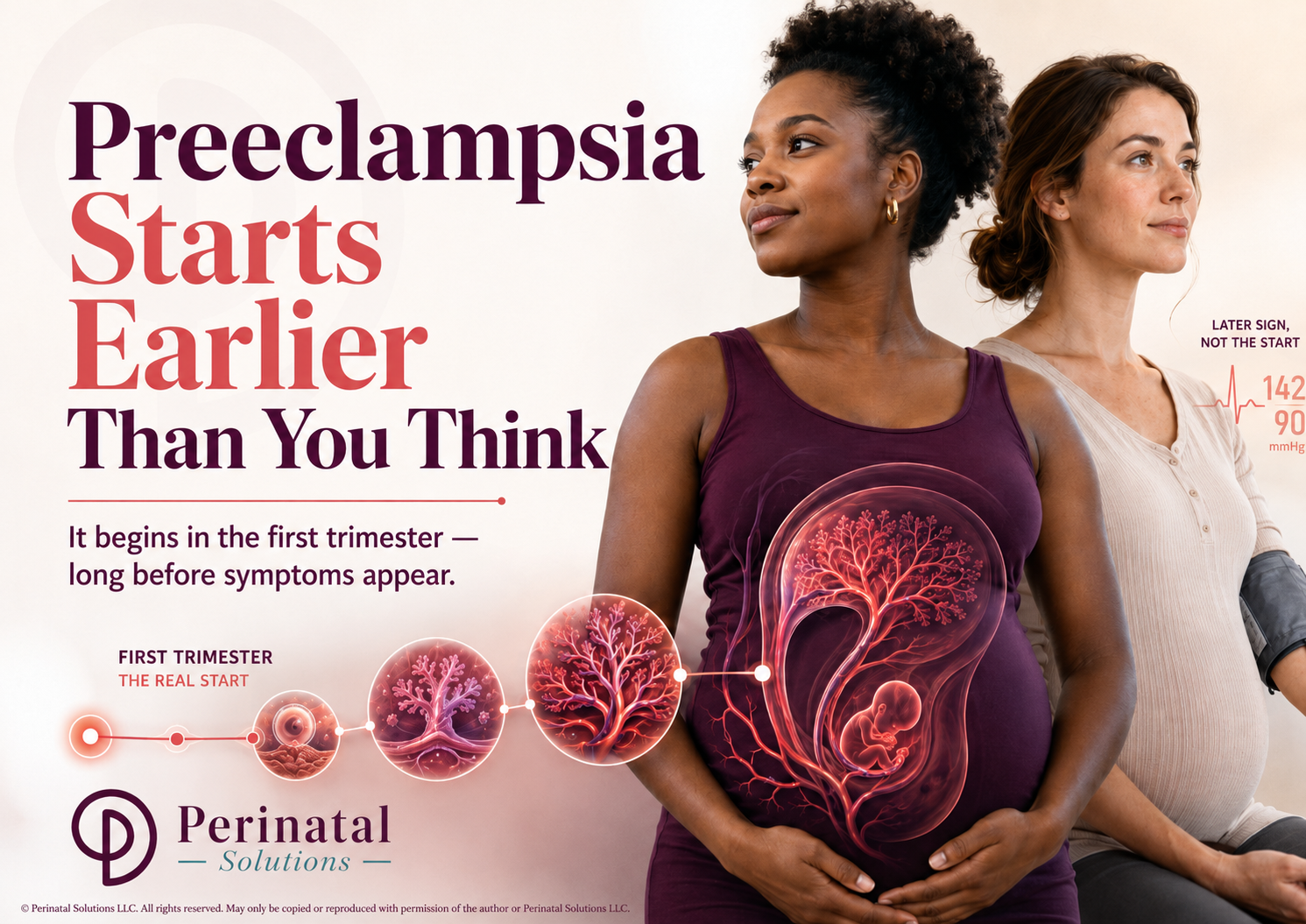
Preeclampsia no longer requires protein in the urine. That was the old rule. Today, if you have a new headache that will not go away, vision changes, pain in your upper right abdomen, or abnormal lab values, that can be preeclampsia. The absence of protein does not mean you are safe.
Low-dose aspirin is now the standard of care for high-risk patients. It should start between 12 and 16 weeks and continue until delivery. If no one has discussed this with you and you have risk factors, ask at your next visit.
When blood pressure reaches 160 over 110, treatment must happen within 30 to 60 minutes. That is not a guideline suggestion. That is the standard. A delay at that level is a system failure.
A new biomarker test received FDA clearance in 2025. The sFlt-1 and PlGF ratio test is now a complementary diagnostic tool for hospitalized patients. This was not available when I wrote the original chapter.
Postpartum monitoring has been formalized. The current standard includes 72-hour inpatient monitoring after delivery and a follow-up visit within 7 to 10 days. Remote blood pressure monitoring programs are now in place at many major centers. The postpartum period is no longer being treated as an afterthought, at least in institutions that are paying attention.
Black Women’s Statistics Have Worsened
Black women experience maternal mortality at more than three times the rate of white women. That gap has not closed. It has persisted through awareness campaigns, task forces, and public pledges. At the same time, the CDC and Maternal Mortality Review Committees have determined that more than 80 percent of pregnancy-related deaths in the United States are preventable. Read that again. Preventable. Given that Black women bear a disproportionate share of those deaths, the majority of Black maternal deaths are likely preventable as well. Structural racism and implicit bias are now officially documented as contributing factors, which is an acknowledgment the field resisted for a long time. But documentation without dismantling is not progress. It is a paper trail on a problem we have chosen not to solve.
(Centers for Disease Control and Prevention, 2025)
What Has Not Changed
Women are still leaving hospitals postpartum without understanding that preeclampsia can develop or worsen after delivery. Seizures can occur up to 96 hours after birth. In some cases, up to 23 days. That fact was in my original chapter. It remains one of the least known and most dangerous gaps in patient education today.
Early warning signs are still being missed. Not because the information does not exist. Systems are not built to catch them reliably, and patients are not consistently taught to recognize them.
That is the blindspot. It was there in 2008. It is still there now.
A Note on Why I Am Still Here
I retired from clinical practice. I no longer see patients. But I have never stopped watching this space.
I reviewed maternal morbidity and mortality cases for the federal government for years. I saw what happens when warning signs are documented but not acted on. I saw what happens when patients are dismissed. I saw what happens when systems assume everything is fine because no one thought to look closely enough.
That work changed how I see everything. It is why I built the Pregnancy Blindspots framework. It is why I keep writing. It is why, seventeen years after that first chapter, I am still in this conversation.
The evidence has evolved. The language has sharpened. But the mission is the same.
If you are pregnant or planning to be, know your baseline blood pressure before conception if at all possible. Ask about aspirin at your first prenatal visit if you have any risk factors. Know that preeclampsia does not always announce itself with obvious symptoms. And know that the postpartum period is not the finish line.
If you are a clinician, a hospital leader, or a health system decision-maker, I want to have a different conversation with you, one about where these blindspots live in your workflows and what it would take to close them.
That conversation is exactly what the Pregnancy Blindspots platform was built for.
Subscribe below to stay in this work with me.
Reference
Centers for Disease Control and Prevention. (2025, September 23). Working together to reduce Black maternal mortality. U.S. Department of Health and Human Services.
https://pregnancyblindspots.substack.com/p/get-your-free-pregnancy-blindspots